Guest Blogger: Dr. Drossman on Opioid Misuse in Gastroenterology and Non-Opioid Management of Abdominal Pain
Author:

Douglas Drossman, MD
Gastroenterologist
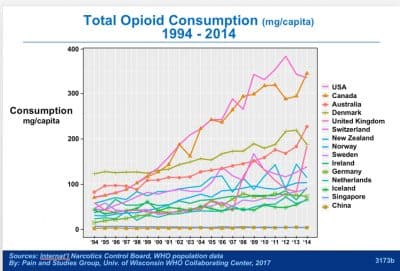
Opioids were one of the earliest classes of medications used for pain across a variety of conditions, but morbidity and mortality have been increasingly associated with their chronic use. Despite these negative consequences, chronic opioid use is increasing worldwide, with the USA and Canada having the highest rates (see figure). Chronic opioid use for non-cancer pain can have particularly negative effects in the gastrointestinal and central nervous systems, including opioid-induced constipation, narcotic bowel syndrome, worsening psychopathology and addiction.
There is no scientific evidence that the use of opioids for chronic non-cancer pain is helpful. In fact, it’s harmful in terms of increased risk of infections and early death. Alarmingly, 70% of IBD patients in hospitals are put on opioids.
How did this misuse happen?
The medical community accepted the use of opioids for non-acute and non-cancer pain beginning in earnest back in 2001 with the Joint Commission’s Pain Standards, which aimed to address the endemic under-treatment of pain.
Now we are facing an opioid crisis, which is the result, in part, of the increased attention to pain management, combined with aggressive marketing and sophisticated delivery systems such as fentanyl patches, which took the focus away from traditional pain control methods such as antidepressants, behavioral interventions, and regional nerve blocks. Additionally, reimbursement by third-party payers also played a role in the US. Thus the traditional treatments of physical therapy, nerve blocks, psychological treatments and antidepressants (all possibly time consuming) were supplanted by quick but expensive delivery systems of opioids.
In light of the current opioid crisis, the Joint Commission is revising its standards on pain assessment and treatment. But it is important to note that there is a misuse of opioids in gastroenterology that can be addressed with a greater understanding of non-opioid management of abdominal pain.
A recent review I co-authored with Eva Szigethy, MD, and Mitchell Knisely, MD, that summarizes the evidence of opioid misuse in gastroenterology, including the lack of evidence of a benefit from these drugs, as well as the risk of harm and negative consequences of opioid use relative to the brain-gut axis.
The review, “Opioid misuse in gastroenterology and non-opioid management of abdominal pain” was published online in Nature Reviews Gastroenterology & Hepatology. doi:10.1038/nrgastro.2017.141
Here are Some Key Points of the Review
- Prescription opioid use is a global epidemic, with substantial increases in opioid-related morbidity and mortality around the world
- There is a lack of evidence supporting the use of opioids for the management of chronic abdominal pain
- Opioid use can have deleterious consequences on the gastrointestinal tract, including opioid-induced constipation (OIC) and narcotic bowel syndrome (NBS)
- Many promising non-opioid pharmacological and nonpharmacological alternatives for treating abdominal pain exist; however, additional research is needed to identify best practices for treating abdominal pain in individuals with gastrointestinal disorders.
- If opioids are prescribed, it is essential to have strategies to monitor and manage opioid misuse, continually monitor risk–benefit clinical profiles, and prevent and treat addiction.
Opioids have been associated opioid induced constipation (OIC) which results from the effects of opioids on nerve receptors of the gastrointestinal tract. It can be treated with man medications to treat constipation or more selective treatments called PAMORAs that block the effects of opioids on the nerves in the gut producing the constipation. However, narcotic bowel syndrome (NBS) is an underrecognized disorder that is growing in frequency due to increased use of opioids in our society. About 5% of patients on opioids end up with NBS and hyperalgesia and paradoxically have worse pain and keep going to the emergency room—and the vicious cycle continues, because they are prescribed more opioids. NBS needs to be identified and the patients taken off narcotic pain control. Rome IV added both of these disorders to their classification system, and they were not there before.
NBS is totally unrelated to OIC. You can have NBS and not be constipated or you can have OIC and not have NBS. Narcotic bowel is increased pain associated with increased use of opioids. And this is a big problem if not recognized as physicians will put patients with abdominal pain on high doses of opioids thus making the pain worse. Some physicians without recognizing NBS are putting patients with abdominal pain on ever higher doses of opioids.
Opioid Management and Alternative Strategies for GI Patients
The review noted above also discusses the guidelines for opioid management and alternative pharmacological and nonpharmacological strategies for pain management in patients with gastrointestinal disorders.
It is important to note that agents such as nonsteroidal anti-inflammatory drugs and cyclooxygenase inhibitors can trigger flares, neuromodulators such as antidepressants, antipsychotics, and anticonvulsants, which down-regulate pain at the brain level, are increasingly being used to counteract pain-related visceral hypersensitivity. Molecular agents such as antagonists to nerve growth factor and transient receptor potential vanilloid receptor subtype 1 and kappa opioid receptor agonists are also being studied.
These may eventually phase out the regular use of narcotics, but importantly, in my opinion, after 40 years of experience and research, there is absolutely no place for opioids in managing chronic abdominal or IBD pain.
Since chronic pain is complex and involves emotional and social factors, a multimodal approach targeting both pain intensity and quality of life is best. Behavioral interventions are also helpful.
This is also a societal issue. In a previous study, [access the study] we found that patients could be successfully taken off opioids in only a few days in the hospital and their pain reduced by about 1/3. Furthermore, we followed patients after taking them off narcotics and they continued to better with pain reduced by 2/3 at 3 months. However, at 3 months half the patients were put back on opioids and when this occurred their pain came back. So they go to the ER or their physicians and get more opioids because this condition is not recognized and those patients are back to where they started.
Doctors need to know that opioid misuse is a growing phenomenon that is epidemic in proportion. They need to understand that non-cancer chronic pain should not be treated with opioids and that narcotic bowel is a separate condition. Patients need to be treated by being taken off narcotics.
Final Thoughts
Given the lack of evidence supporting the effectiveness of opioids for managing chronic pain, as well as the debilitating effects of those drugs on both the gastrointestinal and central nervous systems, alternative approaches to pain management in patients with gastrointestinal con-ditions must be employed. Alternatives to prescribing opioids in this population should include non-opioid pharmacological agents, behavioral interventions, strong physician–patient relationships and multidisciplinary team approaches. This Review underscores the need for additional research on non-opioid pharmacological and nonpharmacological interventions, as well as different formulations and/or delivery mechanisms of opioids for treating chronic abdominal pain in patients diagnosed with gastrointestinal disorders to reduce pain intensity, improve quality of life and avoid addiction.

Featured Articles
June 24, 2023
Tenapanor (IBSRELA) for Treatment of IBS-C: Effective Over 26 Weeks
Conventionally, patients with irritable bowel syndrome (IBS) are subgrouped based on their predominant bowel habit. Given the relevance of psychological comorbidity to IBS symptoms, our aim was to explore an alternative approach to subgrouping by incorporating factors beyond stool form and frequency.
June 24, 2023
Let’s talk about your IBS-C symptoms
Since there are different underlying causes of IBS-C, there is no single treatment approach that is right for everyone. This form will help you and your healthcare provider determine whether your current treatment is right for you, or if it makes sense to try a different approach.

June 24, 2023
The Low FODMAP Diet for Irritable Bowel Syndrome (IBS)
Not sure what the low FODMAP diet is or if it is right for you? Get the evidence-based information you need to know before trying this approach from instructor Emily Haller, MS, RDN
June 24, 2023
Stress and Your Gut: Why it Matters in Digestive Conditions
In this FREE WEBINAR, Megan Riehl, PsyD, MA, explains: Why the brain-gut axis matters in GI conditions, how to calm your stomach during times of stress, which digestive conditions respond well to improvements in stress management and more!


Let’s Keep in Touch!
Subscribe to get the latest news and content delivered straight to your inbox.
Listen to our
latest Podcast!
This will close in 20 seconds